Hypervigilance: Definition, Signs, Causes, and Evidence-Based Ways to Regain Safety
You might be doing all the right things. Your life may look settled from the outside. Yet your body stays tense. Your mind scans automatically. Sleep feels light. Focus slips away easily. Even in safe places, you cannot fully relax.
This pattern is known as hypervigilance.
Hypervigilance is not a character flaw, a lack of resilience, or “just anxiety”. It is a learned nervous system response shaped by experience. When understood properly and addressed at its root, it is highly responsive to appropriate therapeutic support.
This article explains hypervigilance clearly, explores its impact on mental and physical health, and outlines evidence-based approaches used in our clinical practice to help the nervous system recalibrate.
With over 20 years clinical experience working with adults, teens and children in Ireland, UK and worldwide.
Summary
Hypervigilance is a state of persistent threat monitoring where the nervous system remains activated despite the absence of immediate danger. It commonly develops after trauma, prolonged stress, childhood adversity, chronic health conditions, or repeated uncertainty. Over time, hypervigilance can disrupt sleep, digestion, concentration, emotional regulation, relationships, pain processing, and immune balance. Evidence-based psychological and nervous-system-informed therapies can reduce hypervigilance by addressing its underlying drivers rather than suppressing symptoms.


What Is Hypervigilance?
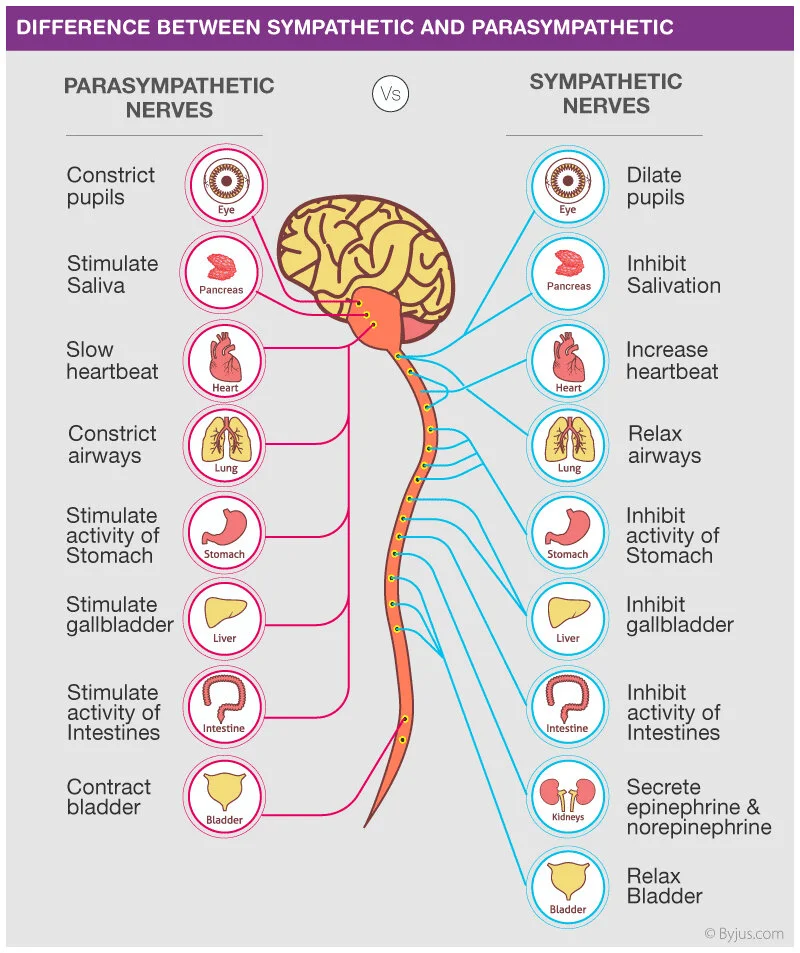
Hypervigilance is a sustained state of heightened alertness characterised by continuous scanning of the environment for potential threat. It is driven by prolonged activation of the autonomic nervous system, particularly the sympathetic branch responsible for fight-or-flight responses.
At a neurobiological level, hypervigilance involves increased reactivity in threat-detection circuits, including the amygdala, alongside reduced regulatory influence from higher cortical regions involved in safety appraisal and emotional regulation.
In simple terms, the nervous system stops checking whether danger is present and begins assuming it is.
This response is adaptive during real threat. It becomes problematic when it persists in everyday life.
Signs and Symptoms of Hypervigilance
Hypervigilance affects the whole system: cognition, emotion, physiology, and behaviour.
Psychological and behavioural signs
- Constantly feeling “on guard”
- Automatic scanning of people, rooms, exits, or surroundings
- Difficulty concentrating, reading, or following conversations
- Heightened startle response to sound or movement
- Irritability, emotional reactivity, or overwhelm
- Difficulty settling at night or maintaining sleep
Physical symptoms
These responses occur automatically, without conscious choice:
- Elevated heart rate or blood pressure
- Shallow or rapid breathing
- Muscle tension, particularly in the jaw, shoulders, and abdomen
- Digestive disturbance including bloating, reflux, or altered bowel habits
- Persistent fatigue or feeling “wired but tired”
Real-world examples
You may always choose seating that allows visual control of exits. Watching television feels difficult because part of your attention is listening for sounds outside. Reading becomes effortful as your focus repeatedly shifts away from the page. These are classic presentations seen clinically.
Hypervigilance vs Paranoia
Hypervigilance and paranoia are often confused but are clinically distinct.
Hypervigilance involves generalised environmental threat monitoring.
Paranoia involves fixed beliefs that specific people or groups intend harm.
Someone experiencing hypervigilance may think, “Something could happen.”
Someone experiencing paranoia may believe, “They are trying to harm me.”
This distinction matters because hypervigilance responds particularly well to nervous-system-focused therapeutic approaches.
Why Hypervigilance Develops
Hypervigilance develops through learning and adaptation. The nervous system adjusts to repeated experiences of threat, unpredictability, or overwhelm.
Common contributing factors
1. Childhood trauma or emotional neglect
Early experiences shape baseline safety perception. Psychological abuse, neglect, or inconsistent caregiving can sensitise threat-detection systems long into adulthood.
2. Prolonged stress and chronic uncertainty
Living for extended periods without predictability teaches the nervous system to remain alert as a protective strategy.
3. Exposure to violence or danger
Community violence, accidents, or repeated frightening events reinforce vigilance patterns.
4. Occupational exposure
Military service, emergency response, healthcare, and high-responsibility roles require sustained alertness that may persist beyond the role itself.
5. Chronic physical health conditions
Autoimmune conditions, chronic pain, gut and digestive disorders, hormonal disruption, fatigue syndromes, and inflammatory states increase bodily uncertainty, reinforcing internal monitoring and threat sensitivity.
How Hypervigilance Affects Daily Life
Relationships and emotional availability
Hypervigilance pulls attention outward, reducing emotional presence. Conversations can feel draining. Neutral cues may be misinterpreted. Over time, this affects trust, intimacy, and communication.
Cognitive function and work capacity
Persistent vigilance creates a feedback loop. Anxiety increases scanning. Scanning increases perceived threat. Cognitive resources are diverted away from planning, creativity, memory, and problem-solving. This commonly affects work, study, and daily functioning.
Physical health and long-term impact
Chronic nervous system activation affects multiple systems:
- Increased cardiovascular strain
- Amplification of pain perception and risk of persistent pain
- Altered gut–brain signalling affecting digestion and appetite
- Disrupted sleep architecture and poor recovery
- Increased inflammatory load over time
Without intervention, these patterns may contribute to long-term health difficulties.
Evidence-Based Ways to Reduce Hypervigilance
Effective support focuses on restoring safety signalling, not forcing relaxation.
Psychological and therapeutic approaches
Approaches commonly used in clinical practice include:
- Counselling and Psychotherapy, to explore how hypervigilance developed and what maintains it
- Cognitive behavioural therapy, ERP, particularly exposure-based approaches that recalibrate threat appraisal
- Hypnotherapy and Clinical Medical Hypnotherapy, working directly with subconscious threat responses
- Rapid Transformational Therapy (RTT), where appropriate, to address core beliefs formed during earlier experiences
These approaches are widely used in presentations involving anxiety disorders, PTSD, panic disorder, chronic stress, health anxiety, and trauma-related conditions.
Practical strategies alongside therapy
- Structured attention-training exercises to rebalance focus
- Reducing exposure to environments or media that maintain threat activation
- Sensory grounding techniques to interrupt automatic scanning
If you have medical conditions or take prescribed medication, consult your GP before making changes.
When Professional Support Is Important
Consider seeking professional support if hypervigilance:
- Interferes with work, education, or daily tasks
- Disrupts sleep most nights
- Strains relationships or emotional availability
- Leads to avoidance of previously manageable situations
- Persists despite self-directed strategies
Early intervention improves outcomes and reduces long-term impact.
Specialist Support at Claire Russell Therapy
At clairerusselltherapy, hypervigilance is understood as a nervous system response shaped by experience, not a personal failing.
With over 20 years of clinical experience, support integrates Counselling, Psychotherapy, Hypnotherapy, Clinical Medical Hypnotherapy, RTT, and Registered Nutritionist services where relevant. Work is tailored for adults, teenagers, and children, addressing psychological, neurological, and physiological drivers together.
Appointments are available ONLINE and in person in Adare, Newcastle West, Limerick, Abbeyfeale, Charleville, Midleton, Youghal, Cork, Dublin, and Dungarvan.
Frequently Asked Questions
Is hypervigilance a diagnosis?
No. It is a symptom pattern seen across anxiety- and trauma-related conditions.
Can hypervigilance improve after many years?
Yes. The nervous system remains adaptable throughout life.
Is hypervigilance linked to ADHD or neurodivergence?
It can be. Heightened sensory sensitivity may increase vulnerability under stress.
Does hypervigilance affect digestion and gut health?
Yes. Chronic stress alters gut–brain signalling and digestive function.
Is online therapy effective for hypervigilance?
Yes. Many clients respond well to online psychotherapy and hypnotherapy.
Is medication always necessary?
No. Many people benefit from therapy alone or alongside medical care.
Book a Consultation Now
Living in constant alertness is exhausting. It is also changeable.
Professional, evidence-based support can help your nervous system relearn steadiness and safety.
Book a Consultation Now
ONLINE or in person in Adare, Newcastle West, Limerick, Abbeyfeale, Charleville, Kanturk, Midleton, Youghal, Cork, Dublin, & Dungarvan.
Academic References
-
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation. Central role of the brain. Physiological Reviews, 87(3), 873–904.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181836/ -
Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J., & Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies. Implications for heart–brain interactions. Neuroscience & Biobehavioral Reviews, 36(2), 747–756.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5573569/ -
Shin, L. M., Rauch, S. L., & Pitman, R. K. (2006). Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Annals of the New York Academy of Sciences, 1071, 67–79.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4561628/ -
Freeman, D., Garety, P. A., Kuipers, E., Fowler, D., & Bebbington, P. E. (2002). A cognitive model of persecutory delusions. British Journal of Clinical Psychology, 41(4), 331–347.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3218073/ -
Teicher, M. H., Samson, J. A., Anderson, C. M., & Ohashi, K. (2016). The effects of childhood maltreatment on brain structure, function, and connectivity. American Journal of Psychiatry, 173(6), 552–561.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6428430/ -
McDonald, C. C., Deatrick, J. A., Kassam-Adams, N., & Richmond, T. S. (2011). Community violence exposure and posttraumatic stress symptoms in adolescents. Journal of Adolescent Health, 49(2), 163–169.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6299456/ -
Adler, A. B., Castro, C. A., & McGurk, D. (2009). Time-driven battlemind psychological debriefing. Military Medicine, 174(1), 21–28.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3182008/ -
Heeren, A., & McNally, R. J. (2016). An integrative network approach to social anxiety disorder. Clinical Psychology Review, 47, 21–33.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2921726/ -
Bar-Haim, Y., Lamy, D., Pergamin, L., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2007). Threat-related attentional bias in anxious and nonanxious individuals. Psychological Bulletin, 133(1), 1–24.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181681/ -
Bishop, S. J. (2009). Trait anxiety and impoverished prefrontal control of attention. Nature Neuroscience, 12(1), 92–98.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3263399/ -
Crombez, G., Vlaeyen, J. W., Heuts, P. H., & Lysens, R. (1999). Pain-related fear is more disabling than pain itself. Pain, 80(1–2), 329–339.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3718611/ -
Steptoe, A., & Kivimäki, M. (2013). Stress and cardiovascular disease. Nature Reviews Cardiology, 9(6), 360–370.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5573569/ -
Finan, P. H., Goodin, B. R., & Smith, M. T. (2013). The association of sleep and pain. Sleep Medicine Reviews, 17(6), 509–519.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5449130/ -
Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3584580/ -
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged exposure therapy for PTSD. Journal of Anxiety Disorders, 21(2), 225–236.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3906827/ -
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy. Behaviour Research and Therapy, 58, 10–23.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3031320/ -
Arnsten, A. F. T. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience, 10(6), 410–422.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6520897/ -
Walker, M. P., & van der Helm, E. (2009). Overnight therapy. The role of sleep in emotional brain processing. Psychological Bulletin, 135(5), 731–748.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7003701/ -
Mayer, E. A., Savidge, T., & Shulman, R. J. (2014). Brain–gut microbiome interactions and functional bowel disorders. Gastroenterology, 146(6), 1500–1512.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6378208/ -
Dantzer, R., O’Connor, J. C., Freund, G. G., Johnson, R. W., & Kelley, K. W. (2008). From inflammation to sickness and depression. Nature Reviews Neuroscience, 9(1), 46–56.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5900333/ -
Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotion regulation. Journal of Affective Disorders, 61(3), 201–216.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6995891/ -
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52(12), 1048–1060.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7468698/ -
Yehuda, R., & LeDoux, J. (2007). Response variation following trauma. Biological Psychiatry, 61(4), 305–314.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7473257/ -
Kim, E. J., Pellman, B., & Kim, J. J. (2015). Stress effects on the hippocampus. Learning & Memory, 22(9), 411–416.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8222874/ -
Slavich, G. M., & Irwin, M. R. (2014). From stress to inflammation and major depressive disorder. Psychological Bulletin, 140(3), 774–815.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8706030/-
McEwen, B. S., & Morrison, J. H. (2013). The brain on stress. Vulnerability and plasticity of the prefrontal cortex over the life course. Neuron, 79(1), 16–29.
https://www.sciencedirect.com/science/article/pii/S0896627313005537 -
Arnsten, A. F. T. (2015). Stress weakens prefrontal networks. Molecular insults to higher cognition. Nature Neuroscience, 18(10), 1376–1385.
https://www.nature.com/articles/nn.4087 -
van der Kolk, B. A. (2014). Developmental trauma disorder. Toward a rational diagnosis for children with complex trauma histories. Psychiatric Annals, 35(5), 401–408.
https://www.healio.com/psychiatry/journals/psycann/2005-5-35-5/%7B7c9bcbcb-9f7f-4b67-9eaa-6c9f6d10cdb7%7D/developmental-trauma-disorder -
Pollak, S. D., & Tolley-Schell, S. A. (2003). Selective attention to facial emotion in physically abused children. Journal of Abnormal Psychology, 112(3), 323–338.
https://psycnet.apa.org/record/2003-06501-002 -
Bishop, S. J. (2007). Neurocognitive mechanisms of anxiety. An integrative account. Trends in Cognitive Sciences, 11(7), 307–316.
https://www.sciencedirect.com/science/article/pii/S1364661307001346 -
LeDoux, J. E., & Pine, D. S. (2016). Using neuroscience to help understand fear and anxiety. American Journal of Psychiatry, 173(11), 1083–1093.
https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2016.16030353 -
Holmes, E. A., et al. (2018). The Lancet Psychiatry Commission on psychological treatments research in tomorrow’s science. The Lancet Psychiatry, 5(3), 237–286.
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(17)30513-8/fulltext -
Shields, G. S., Sazma, M. A., & Yonelinas, A. P. (2016). The effects of acute stress on core executive functions. Journal of Experimental Psychology: General, 145(7), 795–817.
https://psycnet.apa.org/record/2016-18917-001 -
Porges, S. W. (2009). The polyvagal theory. New insights into adaptive reactions of the autonomic nervous system. Cleveland Clinic Journal of Medicine, 76(Suppl 2), S86–S90.
https://www.ccjm.org/content/76/Suppl_2/S86 -
Sterling, P., & Eyer, J. (1988). Allostasis. A new paradigm to explain arousal pathology. In Handbook of Life Stress, Cognition and Health. John Wiley & Sons.
https://onlinelibrary.wiley.com/doi/10.1002/9780470980342.ch9 -
Kim, J. J., & Diamond, D. M. (2002). The stressed hippocampus, synaptic plasticity and lost memories. Nature Reviews Neuroscience, 3(6), 453–462.
https://www.nature.com/articles/nrn849 -
Yehuda, R., et al. (2015). Post-traumatic stress disorder. Nature Reviews Disease Primers, 1, Article 15057.
https://www.nature.com/articles/nrdp201557 -
Lupien, S. J., McEwen, B. S., Gunnar, M. R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, 10(6), 434–445.
https://www.nature.com/articles/nrn2639 -
Hammen, C. (2015). Stress and depression. Old questions, new approaches. Current Opinion in Psychology, 4, 80–85.
https://www.sciencedirect.com/science/article/pii/S2352250X15000371 -
Critchley, H. D., & Harrison, N. A. (2013). Visceral influences on brain and behaviour. Neuron, 77(4), 624–638.
https://www.sciencedirect.com/science/article/pii/S0896627313000704 -
Quigley, E. M. M. (2017). Microbiota–brain–gut axis and neurodegenerative diseases. Current Neurology and Neuroscience Reports, 17(12), 94.
https://link.springer.com/article/10.1007/s11910-017-0802-6 -
Bremner, J. D. (2006). Traumatic stress. Effects on the brain. Dialogues in Clinical Neuroscience, 8(4), 445–461.
https://www.dialogues-cns.org/article/traumatic-stress-effects-on-the-brain/ -
Hayes, J. P., VanElzakker, M. B., & Shin, L. M. (2012). Emotion and cognition interactions in PTSD. Progress in Brain Research, 195, 179–193.
https://www.sciencedirect.com/science/article/pii/B9780444537027000120 -
Schore, A. N. (2001). Effects of a secure attachment relationship on right brain development. Infant Mental Health Journal, 22(1–2), 7–66.
https://onlinelibrary.wiley.com/doi/10.1002/1097-0355(200101/04)22:1%3C7::AID-IMHJ2%3E3.0.CO;2-N -
Danese, A., & McEwen, B. S. (2012). Adverse childhood experiences, allostasis, and allostatic load. Physiology & Behavior, 106(1), 29–39.
https://www.sciencedirect.com/science/article/pii/S003193841100429X
-